
Cancer breakthroughs at ASCO
What we're reading spotlight

We’re experimenting with a different format where we occasionally spotlight a slightly longer What we’re reading post. Our regular roundup from earlier this week is posted here.

There have been lots of big breakthroughs in cancer treatment recently, so I was excited to follow the news from the American Society of Clinical Oncology conference (ASCO 2026), which took place in Chicago this week1, and wanted to share some of my highlights.
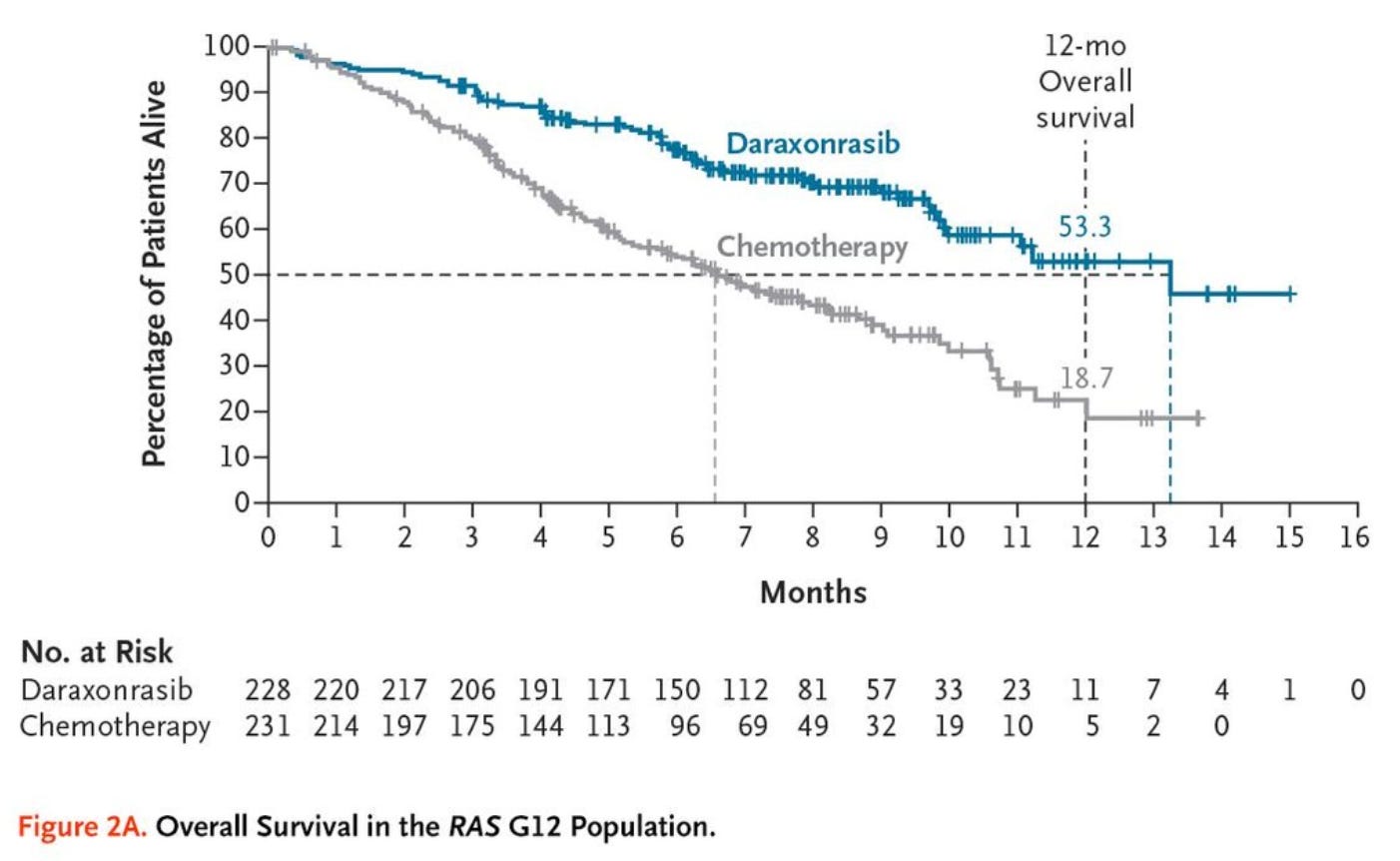
The biggest was daraxonrasib, a new drug against pancreatic cancer. Pancreatic cancer is one of the deadliest, and it has been considered essentially untreatable for a long time, with 5-year survival rates of only ~13%. In a phase 3 trial, daraxonrasib roughly doubled median survival among people with metastatic pancreatic cancer (to about 13 months). This is probably only the beginning, since the drug targets a cancer protein (KRAS) that’s also common in cancers of other organs, including the lungs. Ruxandra Teslo wrote a great piece on how the breakthrough came about here.
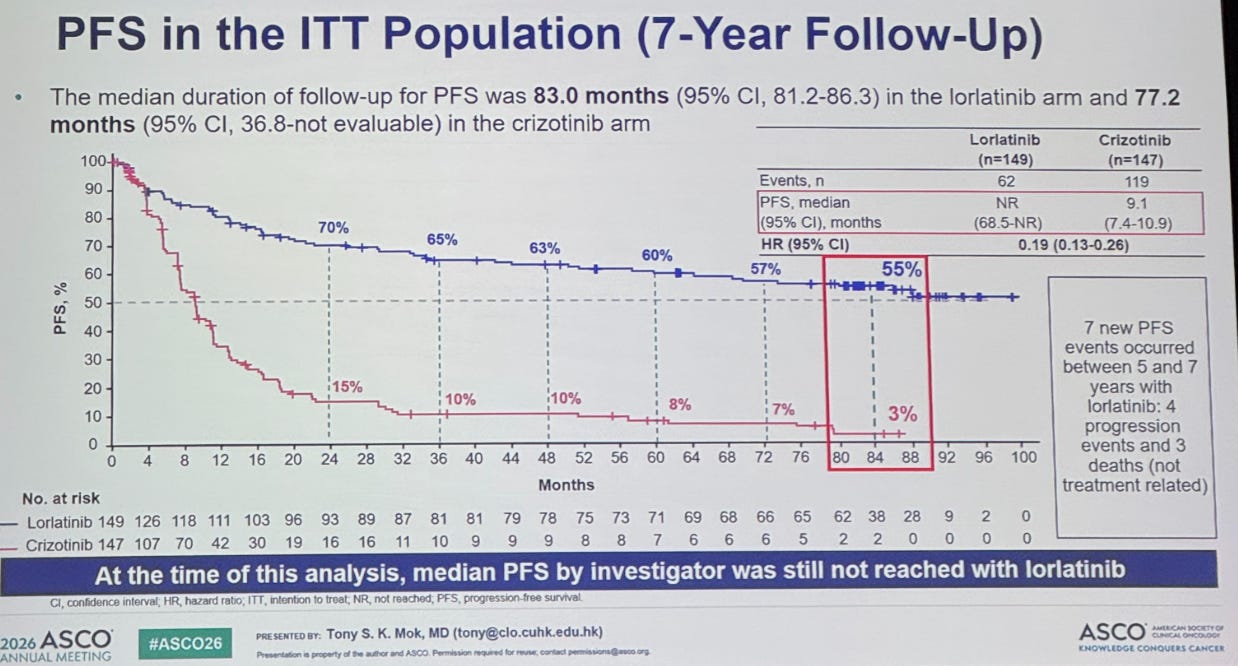
Then there were 7 year results for lorlatinib, a precision drug for metastatic lung cancers: specifically, a type (ALK-positive) that’s common in non-smokers. You can see the results of the phase 3 trial below: 55% of patients were still progression-free after 7 years, versus just 3% on the older drug crizotinib. I have never seen a survival curve like it.
A new prostate cancer drug, talazoparib, cut the risk of progression by about half when added to hormone therapy, compared to hormone therapy alone, in a phase 3 trial for prostate cancers carrying specific DNA repair gene mutations. Talazoparib belongs to a class of drugs (PARP inhibitors) that have already advanced treatment of breast and ovarian cancers with BRCA mutations. This trial suggests the same strategy also works for prostate cancer.

There was also long-term data on a recent endometrial cancer drug, dostarlimab, an antibody that was approved in 2023. After 4 years on the phase 3 RUBY trial, 58% of patients whose tumours carried a ‘mismatch repair deficient’ signature still hadn’t progressed when the drug was added to chemotherapy, versus just 16% on chemotherapy alone. That’s a huge difference! The drug is a checkpoint inhibitor: T cells have built-in ‘checkpoints’ that hold them back from attacking cells unnecessarily, but tumours exploit these to avoid being attacked, so blocking the checkpoint frees the T cells to go after the tumour.
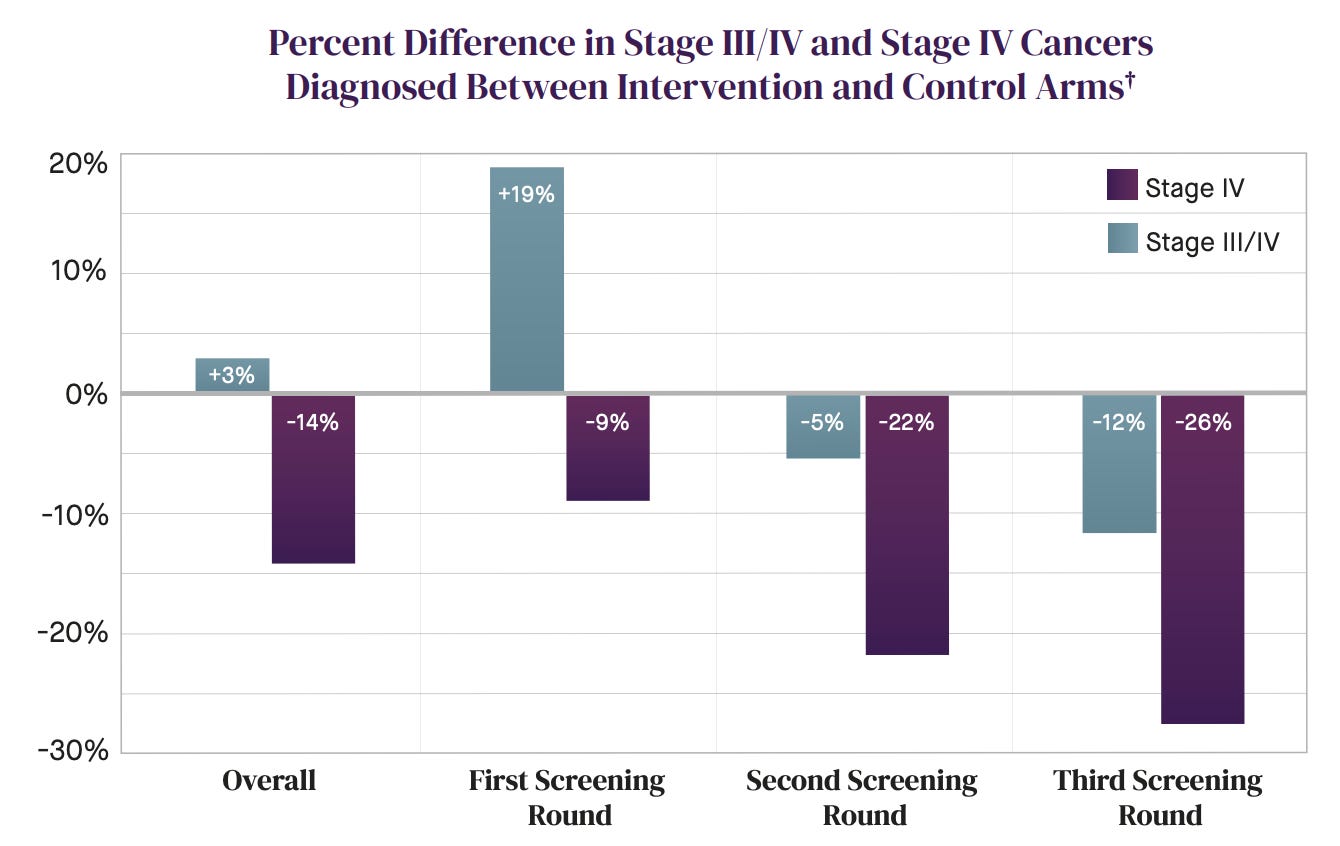
An early cancer detection blood test2, the NHS Galleri blood test, was tested in a large RCT in England with about 142,000 people. The results are a little confusing, so let me start by describing a ‘good result’ in this scenario: detecting a non-benign cancer that would’ve missed otherwise, or catching one earlier so treatment could start sooner.
On the first, it succeeded: roughly quadrupling the detection rate and cutting cancers caught only at emergency presentation by around a quarter. On the second, it detected some cancers earlier: with a 16% rise at stage I–II, and 14% reduction at stage IV. But the trial missed its primary goal: there was no significant drop in combined stage III and IV cancers, because stage III diagnoses rose more than expected and cancelled out the stage IV reduction. The way I’d interpret it all – since the largest jump in detection was at stage III and the combined late-stage count barely changed – is that the ‘early’ detection test was mostly catching cancers at stage III, rather than genuinely early. That may still be useful, of course.
And finally, an mRNA cancer vaccine that might actually work! In people with high-risk melanoma, who’ve already undergone surgery, it cut the risk of cancer recurrence or death by around half, compared to Keytruda (the blockbuster cancer immunotherapy drug) alone, in a phase 2b trial over 5 years.
As I’ve learnt from Ruxandra, many previous mRNA cancer vaccines have been doomed by how they pick their targets. They sequence a tumour’s mutations and design the vaccine against the resulting ‘neoantigens’ (newly formed mutant proteins in a cancer cell), but in many cancers, those neoantigens are never actually displayed on the cell surface, so immune cells can’t recognize them. Melanoma is different: its neoantigens are readily displayed and recognized, which is why drugs like Keytruda already work well against it, and why a vaccine has a much better chance of working as well.
We’re living through a very special time in cancer research.
Sadly I wasn’t there in person, but I still followed along vicariously through everyone else’s posts on social media.
Early cancer detection blood tests always make my spidey senses tingle, so I had to look into this one.
Totally agree with your read on Galleri! Also out last weekend in JAMA... higher diagnostic delay rates during the NHS-Galleri trial, likely because of lack of healthcare abundance (NHS had limited capacity to provide timely follow-up tests). Article here: https://jamanetwork.com/journals/jama/fullarticle/2849767
hi and thank you for this selection. Can I ask: when you write "Melanoma is different: its neoantigens are readily displayed and recognized, which is why drugs like Keytruda already work well against it", what do you mean exactly? Why exactly is Keytruda working well?